
Abstract
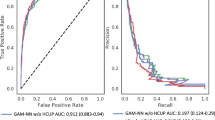
As many as 14 % of patients undergoing coronary artery bypass surgery are readmitted within 30 days. Readmission is usually the result of morbidity and may lead to death. The purpose of this study is to develop and compare statistical and genetic programming models to predict readmission. Patients were divided into separate Construction and Validation populations. Using 88 variables, logistic regression, genetic programs, and artificial neural nets were used to develop predictive models. Models were first constructed and tested on the Construction populations, then validated on the Validation population. Areas under the receiver operator characteristic curves (AU ROC) were used to compare the models. Two hundred and two patients (7.6 %) in the 2,644 patient Construction group and 216 (8.0 %) of the 2,711 patient Validation group were re-admitted within 30 days of CABG surgery. Logistic regression predicted readmission with AU ROC = .675 ± .021 in the Construction group. Genetic programs significantly improved the accuracy, AU ROC = .767 ± .001, p < .001). Artificial neural nets were less accurate with AU ROC = 0.597 ± .001 in the Construction group. Predictive accuracy of all three techniques fell in the Validation group. However, the accuracy of genetic programming (AU ROC = .654 ± .001) was still trivially but statistically non-significantly better than that of the logistic regression (AU ROC = .644 ± .020, p = .61). Genetic programming and logistic regression provide alternative methods to predict readmission that are similarly accurate.



Similar content being viewed by others

References
Stewart RD, Campos CT, Jennings B, Lollis SS, Levitsky S, Lahey SJ. Predictors of 30-day hospital readmission after coronary artery bypass. Ann Thorac Surg. 2000;70:169–74.
Lahey SJ, Campos CT, Jennings B, Pawlow P, Stokes T, Levitsky S. Hospital readmission after cardiac surgery. Does “fast track” cardiac surgery result in cost saving or cost shifting? Circulation. 1998;98:II35–40.
Hannan EL, Racz MJ, Walford G, Ryan TJ, Isom OW, Bennett E, Jones RH. Predictors of readmission for complications of coronary artery bypass graft surgery. JAMA. 2003;290:773–80.
Steuer J, Blomqvist P, Granath F, Rydh B, Ekbom A, de Faire U, Ståhle E. Hospital readmission after coronary artery bypass grafting: are women doing worse? Ann Thorac Surg. 2002;73:1380–6.
Vaccarino V, Lin ZQ, Kasl SV, Mattera JA, Roumanis SA, Abramson JL, Krumholz HM. Gender differences in recovery after coronary artery bypass surgery. J Am Coll Cardiol. 2003;41:307–14.
Zitser-Gurevich Y, Simchen E, Galai N, Braun D. Prediction of readmissions after CABG using detailed follow-up data: the Israeli CABG study (ISCAB). Med Care. 1999;37:625–36.
Koza JR. Genetic programming. Cambridge: MIT press; 1992.
Jacob C. Illustrating evolutionary computation with Mathematica. San Francisco: Academic Press; 2001.
Biesheuvel CJ, Siccama I, Grobbee DE, Moons KG. Genetic programming outperformed multivariable logistic regression in diagnosing pulmonary embolism. J Clin Epidemiol. 2004;7:551–60.
Engoren M, Plewa M, O’Hara D, Kline JA. Evaluation of capnography using a genetic algorithm to predict PaCO2. Chest. 2005;127:579–84.
Engoren M, Kline JA. Use of genetic programming to diagnose venous thromboembolism in the emergency department. Genet Program Evolv Mach. 2008;9:39–51.
Kotini A, Anninos P, Anastasiadis AN, Tamiolakis D. A comparative study of a theoretical neural net model with MEG data from epileptic patients and normal individuals. Theor Biol Med Model. 2005;2:37.
Veltri RW, Chaudhari M, Miller MC, Poole EC, O’Dowd GJ, Partin AW. Comparison of logistic regression and neural net modeling for prediction of prostate cancer pathologic stage. Clin Chem. 2002;48:1828–34.
Liu Y, Khoshgoftaar TM. 2004. Reducing overfitting in genetic programming models for software quality classification. In: Proceedings of the eighth IEEE symposium on international high assurance systems engineering 54–65.
Scott MJJ, Niranjan M, Prager RW. Realisable classifiers: improving operating performance on variable cost problems. In: Lewis PH, Nixon MS, editors. Ninth British machine vision conference. 1998. p. 304–15.
Efron B, Tibshirani RJ. An introduction to the bootstrap. New York: Chapman and Hall; 1993.
Hanley JA, McNeil BJ. A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology. 1983;148:839–43.
Hannan EL, Zhong Y, Lahey SJ, Culliford AT, Gold JP, Smith CR, Higgins RSD, Jordan D, Wechsler A. 30-Day readmissions after coronary artery bypass graft surgery in New York State. JACC Cardiovasc Interv. 2011;4:569–76.
Murphy BM, Elliott PC, Le Grande MR, Higgins RO, Ernest CS, Goble AJ, Tatoulis J, Worcester MU. Living alone predicts 30-day hospital readmission after coronary artery bypass graft surgery. Eur J Cardiovasc Prev Rehabil. 2008;15:210–5.
Tully PJ, Baker RA, Turnbull D, Winefield H. The role of depression and anxiety symptoms in hospital readmissions after cardiac surgery. J Behav Med. 2008;31:281–90.
Oxlad M, Stubberfield J, Stuklis R, Edwards J, Wade TD. Psychological risk factors for cardiac-related hospital readmission within 6 months of coronary artery bypass graft surgery. J Psychosom Res. 2006;61:775–81.
Scheier MF, Matthews KA, Owens JF, Schulz R, Bridges MW, Magovern GJ, Carver CS. Optimism and rehospitalization after coronary artery bypass graft surgery. Arch Intern Med. 1999;159:829–36.
McNally P, Loftus BG. Knowledge of statistical methods and their implications for clinical practice: a survey of paediatricians. Ir Med J. 2005;98:240–2.
Lee JL, McNeer JF, Starmer CF, Harris PJ, Rosarti RA. Clinical judgment and statistics. Lessons from a simulated randomized trial in coronary artery disease. Circulation. 1980;61:508–15.
Afessa B, Keegan MT, Gajic O, Hubmayr RD, Peters SG. The influence of missing components of the Acute Physiology Score of APACHE III on the measurement of ICU performance. Intensive Care Med. 2005;31:1537–43.
Perez A, Dennis RJ, Gil JF, Rondom MA, Lopez A. Use of the mean, hot deck and multiple imputation techniques to predict outcome in intensive care patients in Colombia. Stat Med. 2002;21:3885–96.
Conflict of interest
No authors have any conflicts of interest or any commercial interests in any product mentioned in the manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
This work was conducted at Mercy St. Vincent Medical Center, 2213 Cherry Street, Toledo, OH 43608.
Appendix
Appendix
Sex |
Race |
Ethnicity |
Age |
Insurance type |
Weight |
Height |
Body mass index |
Body surface area |
Smoking history |
Family history of coronary artery disease |
Comorbities |
Diabetes mellitus |
Hyperlipidemia |
Renal Failure |
Hypertension |
Stroke |
Chronic obstructive pulmonary disease |
Peripheral vascular disease |
Cerebrovascular disease |
Myocardial infarction |
Timing of myocardial infarction |
Stable angina |
Unstable angina |
Arrythmia |
Immune suppression |
New York Heart Association class |
Resuscitation |
Prior coronary intervention |
Prior cardiac surgery |
Prior coronary artery bypass surgery |
Prior valve surgery |
Prior other cardiac surgery |
Medicine use |
Digitalis |
Beta blocker |
Intravenous nitrates |
Anticoagulation |
Diuretics |
Inotropes |
Steroids |
Aspirin |
Insulin |
Oral anti-diabetic |
Number of diseased vessels |
Number of distal arterial grafts |
Number of distal venous grafts |
Internal mammary artery use |
Total number of grafts |
Left main disease |
Ejection fraction |
Status (elective, urgent, emergent, salvage) |
Use of cardiopulmonary bypass |
Perfusion time |
Crossclamp time |
Cardioplegia |
Intraaortic balloon pump use |
Timing of Intraaortic balloon pump use |
Blood products |
Number of complications |
Type of complications |
Reoperation for bleeding |
Reoperation for valve surgery |
Reoperation for graft |
Reoperation for other cardiac surgery |
Reoperation for non-cardiac surgery |
Myocardial infarction |
Deep sternal wound infection |
Thoracotomy infection |
Infection of leg incisions |
Sepsis |
Urinary tract infection |
Permanent stroke |
Temporary stroke |
Coma |
Prolonged mechanical ventilation |
Pulmonary embolism |
Pneumonia |
Renal failure |
Dialysis |
Limb ischemia |
Dissection of iliac or femoral arteries |
Heart block |
Arrest |
Coagulopathy |
Cardiac tamponade |
Gastrointestinal |
Multisystem organ dysfunction |
Atrial fibrillation |
Aortic dissection |
Other |
Postoperative length of stay |
Variables included in the analyses. Definitions of the variables were those in use at the time of the individual patient’s surgery and may differ slightly from the current definitions, which are provided at http://www.sts.org/sites/default/files/documents/Training%20Manual%20Update%208%2012.pdf.
Rights and permissions
About this article
Cite this article
Engoren, M., Habib, R.H., Dooner, J.J. et al. Use of genetic programming, logistic regression, and artificial neural nets to predict readmission after coronary artery bypass surgery. J Clin Monit Comput 27, 455–464 (2013). https://doi.org/10.1007/s10877-013-9444-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10877-013-9444-7